Do Low Serotonin Levels Cause Depression?
…and what actually causes depression.

You’ve probably heard that depression is caused by low serotonin levels in the brain.
However, a paper published in 2022 has, for all intents and purposes, debunked this theory.
This paper is titled “The Serotonin Theory of Depression: A Systematic Umbrella Review of the Evidence.” In it, six researchers reviewed a great amount of data to conclude once and for all that depression isn’t caused by a chemical imbalance involving serotonin.
To some, this research has felt like a victory, with many citing it as evidence that depression is an imaginary illness used to get attention.
To others, it has felt like a confusing blow to everything they understand about their mental health.
With so many mixed reactions to this research, I think it’s important to clear the air about what it does and doesn’t say. In this post, I’m going to do my best to give a summary of what this study found, as well as the implications it has for treating depression.
My goal is to approach this topic with as much humility as possible. Depression is a sensitive topic for many, and science has a long way to go before we fully understand it.
To begin, let’s explore a brief history of where we got the idea that depression is caused by a chemical imbalance.
A History of Modern Depression
In the 1960s, a researcher named Alec Coppen published a paper called “The Biochemistry of Affective Disorders.” In it, he wrote that “5-hydroxytryptamine (AKA “serotonin”) may be an important monoamine in reducing depression…”
Coppen was suggesting that low levels of the chemical serotonin are partially responsible for causing depression. Serotonin occurs naturally throughout the body, primarily in the gut and brain.
To help treat depression, Coppen wrote that “there are certain biochemical changes in the brain which need to be restored before the patient’s clinical condition will improve.” In this statement, Coppen expressed his belief that serotonin levels need to be restored to help a patient overcome depression.
Fast forward to the 1980s. Scientists had accepted the theory that low serotonin levels play a role in depression and began trying to create a drug which could increase serotonin in the brain.
After years of research, the pharmaceutical firm Eli Lilly and Company introduced Prozac to the market. (If you’re interested, you can read a thorough history of how this process happened by clicking here.)
Prozac is a type of drug called a “selective serotonin reuptake inhibitor” (SSRI for short.) There are lots of different SSRIs available for prescription use today.
For a long time, it was thought that SSRIs work by preventing the brain from “recycling” serotonin that was already available, leading to more serotonin and ultimately less depression.
However, scientists have been challenging the idea that low serotonin levels cause depression for years, which brings us to the paper we’re examining in this article.
Debunking the Serotonin Myth of Depression
The type of research the authors conducted is called an umbrella review.
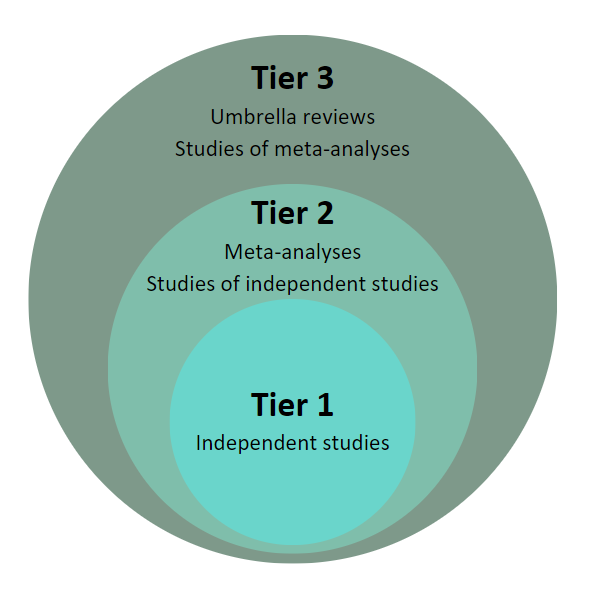
What’s an umbrella review? Well, think about scientific research as existing in three different tiers.
Tier 1 is for independent studies. Scientists publish independent studies all the time, each one contributing a small amount to our overall understanding about a certain topic.
Tier 2 contains “meta-analyses.” Meta-analyses study the independent studies from Tier 1. Researchers gather data from lots of different studies and analyze them together. Meta-analyses are a “study of studies.”
Tier 3 is for “umbrella reviews.” Umbrella reviews gather data from meta-analyses to get an even bigger idea of what research is saying.
Here’s a picture that summarizes these three tiers:
When a researcher conducts an umbrella review well, we can be confident that the results are conclusive. That’s because it’s analyzing data from hundreds, if not thousands, of independent studies.
So, what did this study say about depression?
I think this quote from the paper summarizes it nicely:
“The main areas of serotonin research provide no consistent evidence of there being an association between serotonin and depression, and no support for the hypothesis that depression is caused by lowered serotonin activity or concentrations.”
In case it wasn’t clear, let me summarize: the results from multiple studies with over 300,000 combined participants showed that serotonin doesn’t play a role in depression.
The authors went on to say the following:
“Our comprehensive review of the major strands of research on serotonin shows there is no convincing evidence that depression is associated with, or caused by, lower serotonin concentrations or activity. Most studies found no evidence of reduced serotonin activity in people with depression compared to people without…”
Let that sink in for a moment.
One of the main theories about what causes depression for the past 60 years has been debunked.
So, does that mean that therapists have no idea what causes depression?
Does it mean that SSRIs don’t treat depression?
Does it mean that depression is a fake disorder?
Despite lots of people making these claims, I don’t believe that any of them are true. I’m going to spend the rest of this article answering those questions and hopefully providing some clarity around this confusing topic.
What (Actually) Causes Depression?
I really wish there was a single answer to what causes depression, but unfortunately, research shows that it’s more complex than that.
One of the best papers I’ve read about depression is a meta-analysis that examined the biological, psychological, and social factors that may contribute to depression. For the sake of brevity, I’m going to briefly list some of them. If you’re interested, you can read the full article here.
Biological Factors
Unhealthy gut biomes, which create inflammation that can result in depression
An overactive HPA-axis, which is the body’s stress response system
Cognitive deficits and cognitive decline
Decreases in amygdala volume
Psychological Factors
Neuroticism
Sensitivity to rejection
Shame
Rumination
Social Factors
Experiencing trauma, especially childhood trauma
Socioeconomic status
Food insecurity
Employment status
Lack of close relationships
According to research, it appears that all these factors, among others, often combine to create depression.
It’s also important to note that some people are genetically vulnerable to depression, and that environmental factors can “activate” certain genes to initiate a depressive episode (a process called “epigenetics.”)
As you can see, there’s no one thing that causes depression. Rather, a complex series of interactions between biology, psychology, and the environment make people feel depressed.
The lack of one clear cause of depression leads some to question if depression is a legitimate disorder. However, this lack of clarity is not uncommon.
Take, for example, headaches. Most people have experienced one at some point in their life, but the causes of a headache can vary. Drinking too much coffee, drinking too little coffee, a tense neck or back, dehydration, stress – the causes are endless.
The same can be said for depression. Just like there is no one cause for a headache, there is no one cause of depression.
Do SSRIs Treat Depression?
As a reminder, SSRIs are a type of prescription drug. They are commonly called “antidepressants.”
SSRIs are very common. Data collected between 2015 and 2018 showed that 13.2% of U.S. adults had taken an SSRI in the month prior to being surveyed, making these drugs one of the most popular treatments for depression.
Despite their prevalence, research is mixed about how effective SSRIs are. Some scientists claim that SSRIs are ineffective and unnecessary, while others suggest that they are an essential part of treating depression.
The National Institutes of Health published a helpful summary of the research regarding antidepressants. You can read the full article here.
This article includes several helpful takeaways about antidepressants and depression. Some of them are:
Antidepressants work best with moderate, severe, and chronic depression. People with mild depression aren’t likely to benefit from antidepressants.
Antidepressants provide more relief from depression than placebos, helping about 20 more people per 100 than placebos.
Fewer people who took an antidepressant experience a relapse in depressive symptoms than those who don’t take an antidepressant.
So, we can confidently say that antidepressants provide relief in some cases of depression. The question is, how? If low serotonin levels don’t cause depression, why are SSRIs helpful?
While there’s no single study that fully answers this question, current research suggests several reasons why antidepressants may be helpful in treating depression, including:
Blocking the negative impacts of stress on the brain
Increasing the chemical BDNF, an important chemical in creating and supporting brain cells
Decreasing the impact of stressful life events on people with depression
Reducing inflammation which may account for some depressive symptoms
In short, there are lots of theories about how and why antidepressants are helpful. Despite the scientific community openly acknowledging this, one of the main objections about antidepressants is that we don’t fully understand why they work.
The term “mechanism of action” describes how a drug works on a molecular level. If the mechanism of action about a drug is known, we can explain why it’s effective.
A quick Google search for the medication “Advil” reveals that the exact mechanism of action is unknown. Despite this, few people legitimately think that the pain-relieving effects of Advil are a placebo. I believe that it’s important to have the same standard for potentially life-saving antidepressants.
Additionally, it’s important to remember the intended purpose of antidepressants.
Antidepressants are meant to relieve the symptoms of depression, not treat its source, something that mental health professionals openly acknowledge. It’s comparable to how cold medicine helps relieve a runny nose, fever, and sore throat. The medicine isn’t treating the cause of a cold, but rather the symptoms that make a cold miserable.
It’s also important to acknowledge that the paper which debunked the serotonin myth of depression didn’t study the efficacy of SSRIs. This is important because some professionals claim that this paper proves SSRIs to be ineffective, which simply is not the case.
What Does It Mean to Be Depressed?
As I begin to close this article, I think I be remiss not to discuss what it actually means to “be depressed.”
When someone says that they “struggle with depression,” they are likely referring to experiencing the symptoms of a major depressive episode.
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) is the handbook therapists use to make diagnoses. The DSM-5 is far from perfect and, unfortunately, relies upon clinical observations rather than lab tests to create the criteria for mental health diagnoses.
However, for better or for worse, the DSM-5 is what we use to define a major depressive episode. The criteria is experiencing five or more of the following for the past two weeks:
Depressed mood for most of the day
Reduced interest or pleasure in enjoyable activities
Increased or decreased appetite
Insomnia or hypersomnia
Moving more than usual or being fidgety
Fatigue
Feelings of worthlessness or shame
Difficulty concentrating
Thoughts of death or suicide
If you’re reading these symptoms and believe you’ve experienced them, you’re not alone. Many people struggle with occasional feelings of depression, but this doesn’t necessarily mean they have a mental health disorder.
When diagnosing someone with a depressive disorder, mental health clinicians look at the frequency, intensity, and duration of the symptoms. Someone who occasionally feels sad likely doesn’t meet the criteria of a full-blown depressive disorder.
The difference is that someone with a depressive disorder will have these symptoms more frequently, more intensely, and for a longer period than what is considered “normal.”
As you can probably see, there can be a fine line between sadness and depressive disorders. However, it’s important to take depressive symptoms seriously if they’re beginning to interfere with your daily functioning.
Let me use an analogy to explain. Imagine that you were experiencing a runny nose, fever, and night sweats. After several days, you see a doctor. When they hear about your symptoms, they diagnose you with a common cold and send you home to recover.
However, after resting for a few days, your symptoms begin to worsen. Soon, you can’t breathe out of your nose and your baseline temperature is dangerously high. A follow-up doctors visit and several tests reveal that you actually have an autoimmune disorder, not a common cold.
See why it’s important to have an accurate diagnosis? Not having one can result in worsening symptoms and delayed medical interventions, sometimes making it even more difficult to treat the illness.
Now, I don’t say all of this to argue that everyone who occasionally feels sad has a depressive disorder. Sadness is a normal, and arguably healthy, response to life’s stressors. There may even be times when our culture uses the term “depressed” too loosely, using it to describe a normal reaction to an upsetting event. What I’m asserting is that clinical depression should be taken seriously, just like any other disorder.
Conclusion
We’ve covered a lot in this article, so let me summarize the main points here:
The theory that low serotonin levels cause depression has essentially been debunked.
There are numerous biological, psychological, and social factors that contribute to depression. It’s impossible to pinpoint just one cause for depressive symptoms.
Although they receive criticism, SSRIs can help treat the symptoms of depression; however, they don’t treat the root cause.
People who have occasional symptoms of depression likely don’t meet the full criteria for a depressive disorder. An accurate diagnosis is important because it guides people to the best treatment.
If you’re struggling with symptoms of depression, talk with a doctor or licensed mental health professional. They can help point you in the right direction to begin overcoming your depression.